Beginner’s Guide to Stereotaxic Surgery

Learn More about our Services and how can we help you with your research!
Introduction
Stereotaxic surgery, also known as stereotactic surgery, is a minimally invasive surgical technique used to precisely target areas within the brain. It is commonly employed in neurological research, the treatment of neurological disorders, and various types of biopsies.
The technique was first developed by Horsley and Clarke in the early 1900s for use in non-human primates. This method allows for the precise placement of brain implants, initially ablation electrodes, by utilizing a coordinate system applied to the brain. It wasn’t until 1947 that Spiegel and Wycis adapted this technique and device for use in humans [1].
It is extensively utilized in both preclinical and clinical research. In preclinical animal studies, this technique allows researchers to inject fluids into the brain and stimulate specific brain regions. Clinically, stereotactic neurosurgery is used to treat conditions such as Parkinson’s disease. For example, in a procedure called Pallidotomy, a small electrical probe is inserted into the patient’s globus pallidus, where it is heated to destroy surrounding brain cells and alleviate symptoms [2].
Today, stereotaxy is still widely used, particularly in laboratory animals such as rodents.
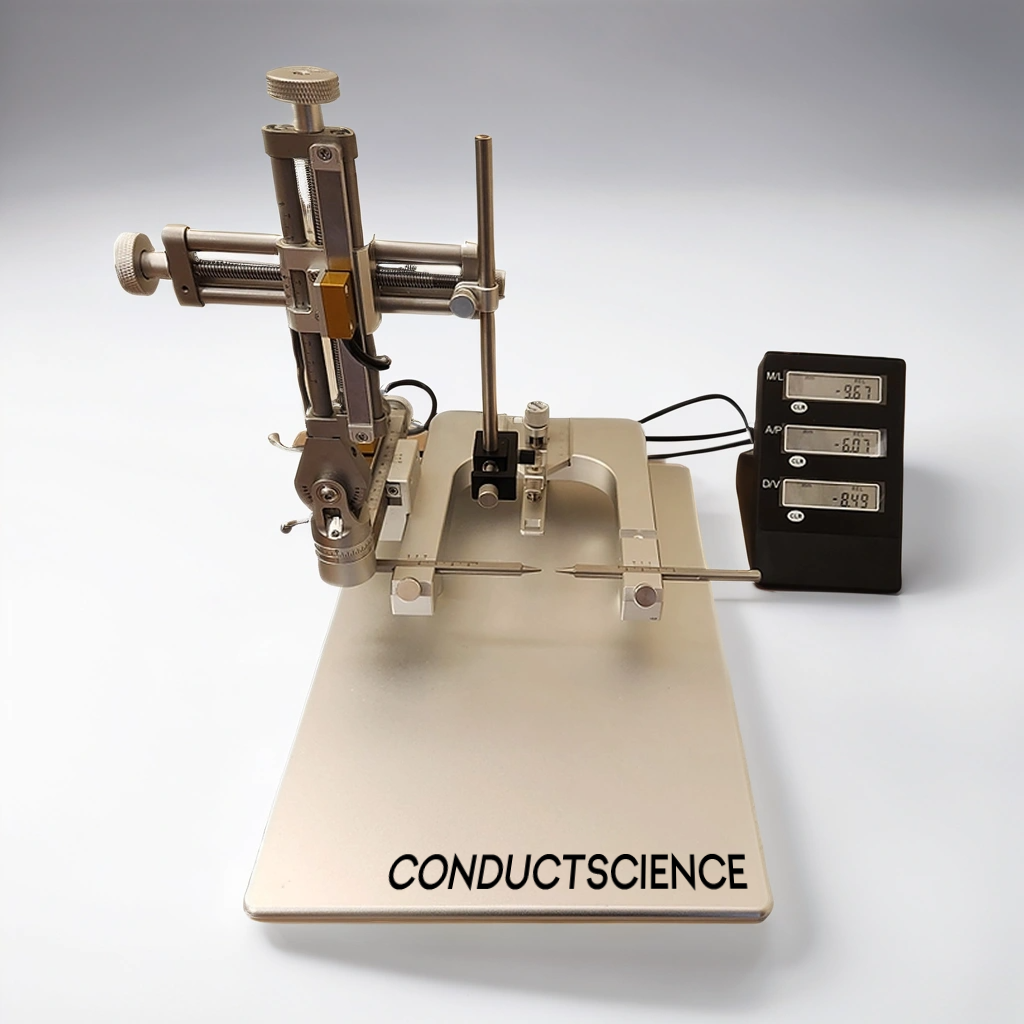
Figure: Stereotaxic Manual Device
Components of the Stereotaxic Apparatus
The stereotaxic apparatus is built around a U-shaped frame mounted on a base plate. This frame supports three mechanical elements that enable precise positioning of an electrode or cannula holder along three orthogonal axes: front-to-back, up-and-down, and side-to-side. The placement of the holder is adjusted using three micrometer Vernier screw drives for fine control.
The apparatus also includes two laterally adjustable ear bars and a height-adjustable incisor bar, which secure the animal’s head in a fixed position. The ear bars align the head parallel to the anteroposterior axis of the frame, while the incisor bar sets the head at the “flat-skull position.” This alignment ensures that the two reference points on the animal’s skull, the bregma and lambda, are on the same horizontal plane, facilitated by the incisor bar.
Step by Step Guide
- Set Up the Stereotaxic Instrument: Prepare all necessary materials, ensuring the area and instruments are thoroughly cleaned and sterilized [3].
- Shave the Fur: Use an electric razor to shave the fur from the ears to just between the eyes, moving in different directions to clean the area effectively. Apply povidone-iodine to the shaved area, avoiding the eyes [3].
- Mount the Animal: Secure the animal onto the stereotaxic apparatus by inserting the ear bars into the ear canal and tightening them. Ensure the head is immobile and level with a ruler. Confirm the 90° angle between the ruler and the animal’s scalp using the stereotaxic instrument [3].
- Make the Incision: Using a sterile scalpel, make an anterior/posterior incision on the scalp from the lambda (a point at the back of the skull) to between the eyes. Pinch the skin with sterilized hemostats to keep the incision open and dry the exposed skull surface with sterile cotton swabs [3].
- Position the Guide Cannula: Mount the guide cannula and locate bregma on the skull. Record the anterior/posterior and lateral coordinates, then find the correct coordinates for probe placement using a stereotaxic atlas. Adjust the guide cannula to the correct coordinates and record the ventral coordinate. Mark the drilling spot on the skull with a sterile pencil [3].
- Drill the Hole: Sterilize the drill bit and carefully drill a hole at the marked location until you penetrate the skull. Ensure the guide cannula can pass through the hole without touching the sides. Use a sterile needle to puncture the meninges for unobstructed cannula insertion [3].
- Prepare for Skull Screws: Using a hand drill, create six holes for skull screws: two anterior, two lateral, and two posterior to the cannula hole. Sterilize the screws and anchor them tightly onto the skull [3].
- Insert the Guide Cannula: Clean the guide cannula with ethanol and saline, then mount and lower it to the proper ventral coordinate, ensuring a perfect vertical insertion without touching the sides [3].
- Secure with Dental Cement: Place an anchor screw medially behind the posterior skull screws. Mix a thin batch of liquid dental cement to cover the guide cannula, screws, and skull. Apply a thicker batch to secure the area, ensuring smoothness to prevent skin irritation [3].
- Finish the Cement Application: As the cement thickens but before it solidifies, separate the skin from the cement cap and mold it to ensure smoothness [3].
- Allow Cement to Dry: Let the dental cement dry completely before removing the animal from the apparatus. Remove the hemostats and apply bacitracin around the cement cap [3].
- Fit the monoinjector to the stereotaxic frame: Lower the needle into the hole to the target DV coordinate and inject. Leave the injection needle in place for at least 30 sec after completion of the injection and before removal of the needle [4].
- Remove the monoinjector and seal the hole with bone wax. Suture the incision and remove the animal from the stereotaxic frame [4].
- Post-Procedure Injections: Administer 0.25 ml of penicillin intramuscularly, followed by 1 ml of saline subcutaneously [3].
- Monitor Recovery: Place the animal in its cage and monitor it until consciousness is regained. Return it to its room for recovery [3].
- Post-Op Monitoring: Check animals daily for signs of infection, pain, or distress until the end of the experiment. Look for low movement, distress vocalization, hunched posture, diarrhea, swelling, discharge, and lack of feeding/drinking. Administer buprenorphine for pain and antibiotics for infections as needed. Euthanize the animal if symptoms persist despite treatment [3].
Figure: Parts of the Stereotaxic Apparatus
Precisely targeting hard-to-reach brain regions remains challenging, especially when dealing with midline brain structures. These challenges involve avoiding critical areas like the superior sagittal sinus and the third ventricle, and consistently targeting specific, discrete brain nuclei. Additionally, advanced neuroscience methods such as optogenetics, fiber photometry, and two-photon imaging require the precise implantation of significant hardware into the brain, with spatial constraints often posing a common obstacle. Study from 2020 (Faber et. al), presented a modifiable protocol for stereotactic targeting of rodent brain structures using an angled coronal approach that may be adapted for 1) either mouse or rat; 2) various neuroscience techniques and 3) for multiple brain regions [5]. You can find a comprehensive description of the protocol in the online article.
Care and Storage
To ensure the longevity and precision of stereotaxic instruments, proper handling and storage are essential. After each surgical procedure, the stereotaxic apparatus and reusable instruments must be cleaned, decontaminated, and sterilized. Initially, wash the instruments with soap and water, thoroughly dry them, and then sterilize them using an autoclave. For more delicate materials such as cannulae, obturators, and electrodes, carefully decontaminate or autoclave them, considering their specific tolerances.
When cleaning the stereotaxic apparatus, use cotton swabs or paper towels soaked in a 70% ethyl alcohol antiseptic solution to clean the frame, ear bars, nose bars, tooth bars, verniers, heating pad, rectal temperature probe, and workbench.
Regular preventive maintenance and servicing of the equipment, based on usage frequency, are crucial for storage. These practices help maintain the instrument’s precision and prevent potential stereotaxic errors caused by loose or unstable components.
References
- De Vloo, P., & Nuttin, B. (2019). Stereotaxy in rat models: Current state of the art, proposals to improve targeting accuracy and reporting guideline. Behavioural brain research, 364, 457–463. https://doi.org/10.1016/j.bbr.2017.10.035
- Laitinen LV, Bergenheim AT, Hariz MI. Leksell’s posteroventral pallidotomy in the treatment of Parkin-son’s disease. Journal of neurosurgery. 1992; 76(1):53–61. https://doi.org/10.3171/jns.1992.76.1.0053
- Geiger BM, Frank LE, Caldera-Siu AD, Pothos EN. Survivable stereotaxic surgery in rodents. J Vis Exp. 2008 Oct 6;(20):880. doi: 10.3791/880. PMID: 19078946; PMCID: PMC3233859.
- Athos, J., & Storm, D. R. (2001). High precision stereotaxic surgery in mice. Current protocols in neuroscience, Appendix 4, . https://doi.org/10.1002/0471142301.nsa04as14
- Faber, C. L., Matsen, M. E., Meek, T. H., Krull, J. E., & Morton, G. J. (2020). Adaptable Angled Stereotactic Approach for Versatile Neuroscience Techniques. Journal of visualized experiments : JoVE, (159), 10.3791/60965. https://doi.org/10.3791/60965
See more of Our Posts
stereotaxic on resources
All Resources
Never miss our posts!
Author:

Louise Corscadden, PhD
Dr Louise Corscadden acts as Conduct Science’s Director of Science and Development and Academic Technology Transfer. Her background is in genetics, microbiology, neuroscience, and climate chemistry.