App concept
PTSD Coach is a smartphone application developed by the U.S. Department of Veterans Affairs for PTSD self-management and self-assessment in symptomatic trauma sufferers. PTSD Coach was designed as a public health tool aimed to decrease the burden of PTSD and increase awareness and availability of PTSD care for trauma sufferers, particularly for war veterans.
The app has four sections available from the main screen: Learn, Track Symptoms, Manage Symptoms and Get Aid. The Learn section contains essential information about PTSD including mechanisms of its development, evidence-based professional care, and the impact of the disorder on the sufferer’s family.
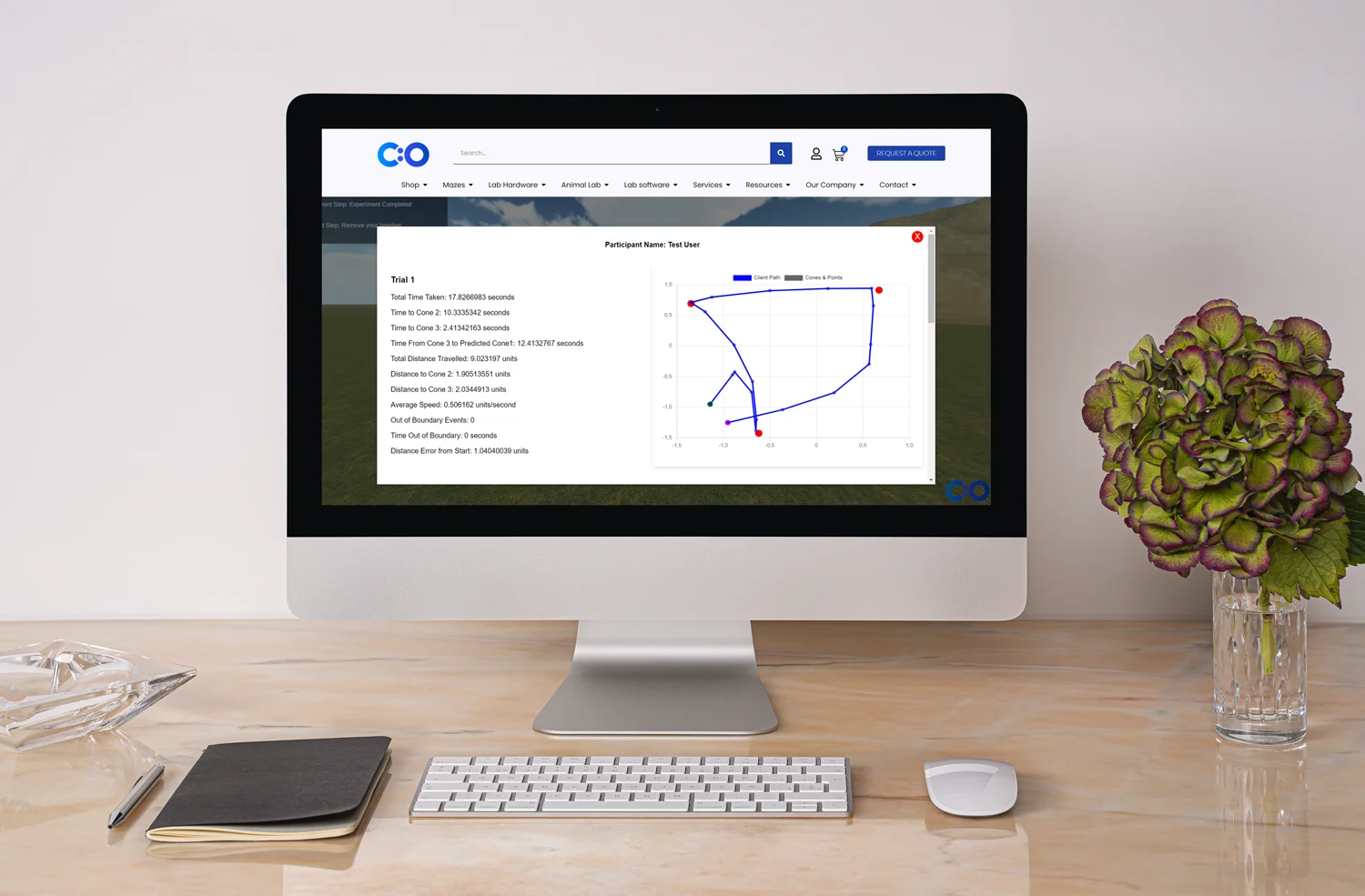
Track Symptoms section allows users to take PCL and receive an interpretation of the symptoms and their severity with advice regarding the type of required treatment. This section can also be used by doctors and researchers are able to obtain data regarding the severity of the patients’ PTSD symptoms.
The Manage Symptoms section offers coping strategies for each type of PTSD symptom. The incorporated coping tools use audio alone (for example, mindfulness meditation sessions) or with images (for example, positive imagery technique) to guide the user during the coping session.
Finally, the Get Aid section contains contacts of support resources and allows for to add of additional supportive contacts such as family members, friends, therapeutists, sponsor etc.
PTSD Coach: studies by Kuhn et al.
PTSD Coach was investigated in a clinical trial which was conducted by Kuhn and colleagues and included 120 participants. 62 of them were randomized to PTSD Coach intervention and 58 were assigned to a waiting list condition and received no care. The outcome was measured at baseline, post-treatment, and 3 months following treatment with PCL, PTSD symptom coping self-efficacy questionnaire, PHQ-8 measuring depression, and Brief Inventory of Psychosocial Functioning. All the measurements and data gatherings were done using the digital versions of questionnaires.
Patients in the PTSD Coach group had clinically and statistically significant improvement in PTSD symptoms than patients in the waitlist group which persisted during the 3-month follow-up; a higher proportion of patients in the PTSD Coach group compared to the waitlist group achieved clinically significant improvement (46.8% vs. 25.9%). [5] The time using the app and pages visited inside the app was also tracked but no significant associations with clinical improvement were found.