x
[quotes_form]
Skip to content
Go
Categories
$
0.00
0
Cart
Request a Quote
Mazes
Close Mazes
Open Mazes
Classic Mazes
Learning Mazes
Anxiety & Depression
Exploration
Motor
Social
Spotlight
Spotlight Anxiety & Depression
Spotlight Exploration
Spotlight Learning & Memory
Spotlight Motor Function
Spotlight Social
Automated
View All Automated
Automated Conditioned Place Preference
Automated Elevated Plus Maze
Automated Hole Board
Automated 8 Arm Radial Maze
Automated T Maze
Automated Y Maze
Rotameter
Operant
Operant Conditioning
Self Administration Chamber
Bussey-Saksida Touch Screen Operant Conditioning Chamber
Empathy Assay
Five Choice Serial Reaction Time Task (5CSRTT)
IDED Operant Chamber
Activity
Activity Cage
General Rodent Activity System
Grip Strength Test
Parallel Rod Test
Repeated Acquisition and Performance Chamber
Rotarod
Treadmill
Metabolic Treadmill
SmartCage System
Conditioning
Active Place Avoidance APA
Active/Passive Avoidance Shuttle Box
Aron’s Test
Fear Conditioning
Learned Helplessness
Vogel’s Test
Step Down Avoidance
Pain & Heat
Electric Von Frey
Hot/Cold Plate
Orofacial Pain Device
Plantar Test Hargreave’s Apparatus
Accesories
Lickometers
Maze Backlight
Olfactory System
Automated Pellet Dispenser
Sound Attenuating Chamber
Video Tracking
ConductVision
AnyMaze
Noldus EthoVision XT
Discover
Historical Mazes
Replication
AeroDeliver System
Labyrinth
Trims
Species
Rodents
Drosophila
Ants
Zebrafish
Pigs
Sheeps
Bats
Bees
Humans
Plants
ConductVision
Close ConductVision
Open ConductVision
Rodent Applications
Barnes
Elevated Plus Maze
Light & Dark
Morris Water
Open Field
T Maze
Radial Arm
Zebrafish Applications
Visual Water Maze
Y Maze
Swim Tunnel Zebrafish
Five Choice Zebrafish
Light and Dark Zebrafish
Advanced Rodent Mazes
APA
Step Down
Automated Y
Social Interaction
RAPC
Fear Conditioning
Drosophila Applications
Heat Maze Drosophila
Visual & Olfatory Apparatus
Drosophila Shallow Chamber
Maze Array Drosophila
Advanced Species
Aquatic Models
Mammalian Models
Insect & Arthropod Models
Avian Models
Reptile & Amphibian Models
Frontier Model Systems
Hardware
Conduct Insecta
Gait Master
Conduct Nest
Video tracking cameras
Advanced Features
Native Hardware Integration
Social Interaction
Autonomous Upgrades and Scalability
NIH Data Management & Sharing (DMS) Compliance
3D Video Tracking
Unsupervised Learning
ConductVision Signal Syn
Advanced Behaviors
Rodent Gait Analysis
Social Interaction
Grooming
Plans & Support
Free Trial
Request a Demo
Conduct Care
Switching Plan
Professional On-Site Training
Species
Rodents
Drosophila
Zebrafish
Lab Hardware
Close Lab Hardware
Open Lab Hardware
Shakers
Multi-functional Shaker: Horizontal + Pendulum+ 3D
Horizontal Shakers
Split Type Shakers
Smart PCR System
Benchtop Instruments
Benchtop Incubators
Dry/Oven Incubators
Centrifuges
Homogenizers
Dry Baths
Syringe & Peristaltic Pumps
Analytical Instruments
Automated Cell Counter
PCR Thermocyclers
Electrophoresis Systems
Imaging Systems
Molecular Biology Accessories
Solid Processing
Imaging & Microscopy
Compound Microscope
Digital Microscope
Stereo Microscope
Specialized Microscopes
Lab Furniture
Ductless Fume Hoods
Safety Cabinets (Flammable/Acid)
Storage Cabinet
Pathology
Pathology Workbench series
Manual Microtome Series
Semi-Automatic Microtome Series
Animal Lab
Close Animal Lab
Open Animal Lab
Surgery & Intervention
Spinal & Cortical Impactor
Weight-Drop TBI Model
Manual Stereotaxic Frame
Digital Stereotaxic Frame
Advanced Stereotaxic
ConductSurgery
Anesthesia & Support
Complete Anesthesia Machine
Induction Chambers
Gas Scavenging Units
Cone Masks
Vaporizer Carts & Parts
Heating & Homeothermic
Homeothermic Monitoring System
Rodent Heating Pad
Thermal Sensor
Pulse Oximeter
Blood-Pressure System
Respiration Monitor
Housing & Handling
Rodent Cages
Broome Restrainers
ArcCage System
Injection Cone w/ Light
Tail Injection Devices
Optogenetics & Photometry
Optogenetic Accesories
Fiber Photometry
Small-Animal MRI
MCAO Stroke Models
Syringe & Peristaltic Pumps
Single Channel
Dual Channel
High precision micro Injection
Manual Micropush Injector
Osmotic pump
Anesthesia Pump
Accesories
Adaptors
Ear Bars
Masks
Holders
Microdrills
Lab Software
Close Lab Software
Open Lab Software
Conductor Software
Features
Request a Demo
Virtual Reality Science
Four Mountains Test
Virtual Morris Water Maze Full Package
Virtual Radial Arm Maze
Virtual Reality Environments
Contact Us (VR)
Software
EthoVision XT
Anymaze
ConductVision
ConductSurgery
ConductSignal
Resources
Close Resources
Open Resources
Learning & Resources
Stories
Protocols
Science
Categories
Scholars Fellowship (CSF)
Education & Fellowships
Academia
Grants
Lab Management
Purchasing Guides
Science
Biomolecules
Data Science
DIY
Electrophysiology
Enzymology
Lab-Basics
Laboratory Techiques
Molecular Genetics
Maze Systems
Labyrinth
Historical Mazes
Maze Replication
Trims
SmartCage System
Digital Health
Mobile Health
Virtual Reality Science
Open Science
Publication Platform
Clinical Tools & Guides
About
Close About
Open About
Our Company
About us
Citations
Customer Stories
Vendor
Shop
Tech Transfer
Publications
Press
Join our affiliate program
Returns & Refunds
Contact
Contact Form
Order Tracking
Book Appointment
Request a quote
Help & Support
Call Us: +1 847 983 3672
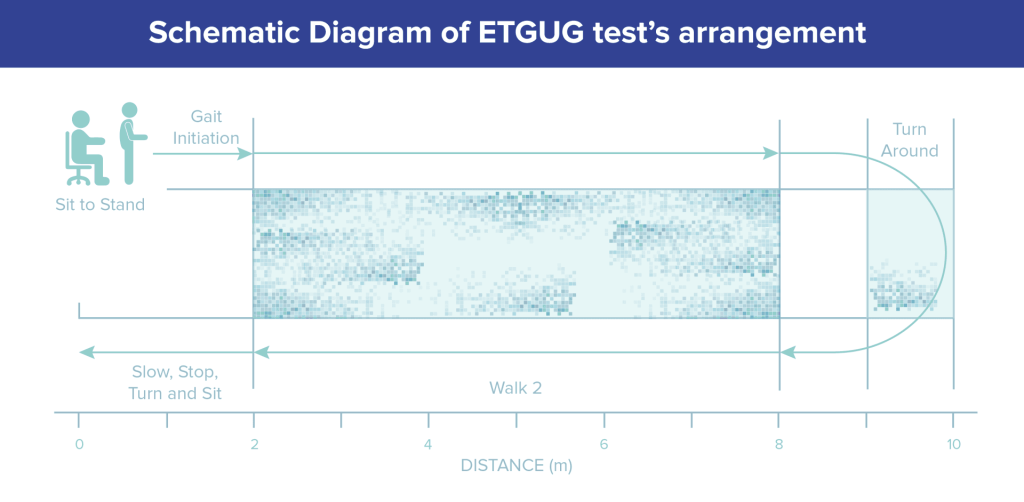
Timed Up and Go Test (TUGT)
Learn More
Get a Quote
About
Documentation
Introduction
Methods
Cosmin Checklist
Strengths and Limitations
Summary and Key Points
References