Description
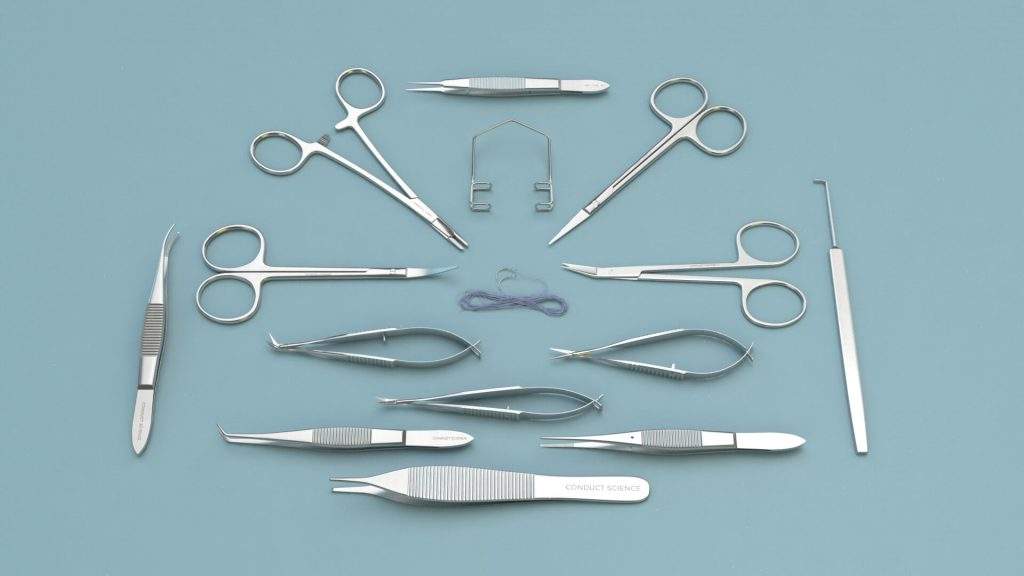
Mouse Kit
| SKU |
Product Description |
Qty |
| S14014-11 |
Operating Scissors (Round Type)-S/S Str/11.5cm |
1 |
| S16014-09 |
NAIL Scissors (Broad Type)-S/S Str/9cm |
1 |
| S21020-14 |
Friedman-Pearson Rongeurs (SGL)-Str/0.7mm Cup/14cm |
1 |
| S22004-11 |
Bone Cutters with Flat Blades (SGL)-11.5cm |
1 |
| S21023-14 |
Friedman-Pearson Rongeurs (SGL)-Cvd/0.7mm Cup/14cm |
1 |
| S23007-12 |
LAMBOTTE Osteotomes – 4mm Cutting Edge/12.5cm |
1 |
| S33006-13 |
GRAEFE Scalpels-22mm Cutting Edge/13cm |
1 |
| SP0000-P |
Instrument Storage Portfolio, 32*22cm |
1 |
Rat Kit
| SKU |
Product Description |
Qty |
| S14014-11 |
Operating Scissors (Round Type)-S/S Str/11.5cm |
1 |
| S16014-09 |
NAIL Scissors (Broad Type)-S/S Str/9cm |
1 |
| S21020-14 |
Friedman-Pearson Rongeurs (SGL)-Str/0.7mm Cup/14cm |
1 |
| S22004-11 |
Bone Cutters with Flat Blades (SGL)-11.5cm |
1 |
| S21023-14 |
Friedman-Pearson Rongeurs (SGL)-Cvd/0.7mm Cup/14cm |
1 |
| S23007-12 |
LAMBOTTE Osteotomes – 4mm Cutting Edge/12.5cm |
1 |
| S33006-13 |
GRAEFE Scalpels-22mm Cutting Edge/13cm |
1 |
| SP0000-P |
Instrument Storage Portfolio, 32*22cm |
1 |
Introduction
Orthopedic surgery is performed to repair bone injuries and improve the quality of life, particularly in older adults. However, the complete understanding of the interactions between factors such as hormone and nutrition status, and underlying cellular mechanisms remains a topic of ongoing research.
Earlier animal models for orthopedic surgery included dogs, sheep, and rabbits, but they had limitations in terms of cost, handling difficulties, and availability of transgenic animals. Rodents, particularly mice, have gained popularity as the preferred model organism due to their shorter breeding cycles, faster regeneration, lower costs, and ease of handling.
Apparatus and Equipment
Before performing the surgical procedure, it is important to ensure that all apparatus and equipment are thoroughly cleaned and sterilized. Instruments that can be autoclaved should be sterilized, and appropriate disinfection methods should be used for other instruments. The operating area should be kept sterile and free of disturbances.
Before the surgery, record subject identification details such as strain and gender, and note the weight of the subject. Perform a physical assessment to evaluate the subject’s health status and activity level. Adequate acclimation of the subject to the facility is necessary, which may take several days to weeks.
Anesthesia is commonly induced in the subject using inhalant agents. Anesthetic systems utilizing a face mask or an anesthetic chamber can be used for induction. The amount and duration of anesthesia induction depend on factors such as the subject’s weight. Verify the depth of anesthesia using appropriate tests, such as the toe pinch test. Monitoring physiological parameters throughout the procedure helps ensure the effectiveness of anesthesia.
Orthopedic Surgery Protocols
Orthopedic studies contribute to the understanding of injuries and the regenerative properties of bones in relation to factors such as age and gender. Reliable rodent models are used for investigations aiming to enhance treatment methods and quality in human orthopedic procedures.
Tibial Fracture Protocol (Xiong Et Al., 2018):
- Place the subject in a supine position on a heated mat.
- Administer analgesia before and after surgical manipulation.
- Perform a skin incision along the medial aspect of the hind limb.
- Visualize the diaphysis and tibial plateau.
- Insert a stainless steel pin into the medullary cavity.
- Induce a fracture at the midshaft of the tibia using Bonn scissors.
- Stabilize the fracture site and close the incision.
Distraction Osteogenesis Protocol (Lybrand Et Al., 2015):
- Position the subject with the operative extremity up.
- Make a longitudinal incision along the femur.
- Expose and dissect muscle fibers attached to the femur.
- Place wires around the femur and secure them with a distraction osteogenesis device.
- Create a transverse osteotomy of the femoral shaft using a circular saw.
- Close the incision and fascia.
Marrow Ablation Protocol (Lybrand Et Al., 2015):
- Place the subject on its back with the operative leg flexed.
- Make an incision over the knee joint and expose the tibial medullary canal.
- Insert spinal needles of increasing diameter to ablate the marrow.
- Flush the bone marrow cavity with sterile saline.
- Close the incision.
Destabilization Of The Medial Meniscus Protocol:
- Position the subject in the supine position.
- Make a skin incision from the patella to the tibial plateau.
- Open the joint capsule and section the meniscotibial ligament.
- Close the wound.
Calvarial Defect Protocol (Spicer Et Al., 2012):
- Induce anesthesia and make an incision over the calvarium.
- Score and remove the calvarium to expose the dura.
- Clean the defect and place the implant material.
- Close the periosteum and skin.
Total Hip Replacement Arthroplasty (Powers Et Al., 1995):
- Make an incision and expose the lateral hip muscles.
- Excise the femoral head and ream the intramedullary cavity.
- Place the femoral component and fix the acetabular component.
- Reduce the hip and close the incision.
Standard Closed Femoral Fracture Protocol (Bonnarens And Einhorn, 1984):
- Flex the knee and make a small incision near the patella.
- Dislocate the patella to expose the femoral condyles.
- Insert a pin retrograde into the femoral canal.
- Cut and bury the pin beneath the bone.
- Fracture the femoral diaphysis by dropping weight.
Post-Operative Care And Pain Management
Pre-emptive measures to avoid postoperative pain in the subject can be done by administering a dose of opioids before incision. After the surgery, the subject must be kept warm in a recovery unit using hot water blankets, hot water bottles, heat pads, and warm sterile saline should also be administered to the subject before returning it to its home cage.
Recovery from anesthesia should be monitored closely and respiratory support, if needed, should be provided. Analgesic should be maintained postoperatively for up to 48 hours in increments of 24 hours or as required. The use of NSAIDs should be avoided as they tend to interfere with the bone healing process. The subject can be returned to its home cage once it has recovered.
Although rare, post-operative prophylactic antibiotics can be administered to prevent infections. Look out for signs of infections such as swelling, lethargy, and purulent drainage. Infection can affect bone healing, thus if an infection is noticed the subject should be euthanized.
Surgery-specific complications and issues may occur post-operatively. Wound dehiscence should be dealt with by re-suturing the wound under anesthesia. If repeated re-suturing fails, allow the wound to heal by secondary intention using an antibiotic ointment. Surgery involving pin placement may have an occurrence of pin slippage. Pin slippage may be visualized outside the skin. Remove the pin using a needle driver. In marrow ablation protocol, tibia fracture risk exists while instrumenting the medullary canal. Tibia fracture may be indicated by the subject’s inability to bear its weight on the operated extremity or by the presence of deformity. In such a situation the subject must be euthanized.
Applications
Micro-computed tomography revealed a transient reduction in fracture size four weeks after the fracture, which reached the control level after weeks 6 and 8. Further, infrared spectroscopy confirmed the involvement of a specific compound in increasing the collagen crosslink ratio, which is linked with improving the biomechanical properties of the fracture callus.
Evaluation of the effects of Nrf2 deficiency in fracture healing
The investigation was conducted using genetically modified mice that lacked a specific protein called Nrf2. These mice were subjected to a standard close femoral shaft fracture, while normal mice were used as a control group for the investigation. Results from the investigation revealed that Nrf2 expression is activated during fracture healing. Analysis data suggested that mice without Nrf2 developed significantly fewer callus tissues and showed delayed bone healing and remodeling compared to the control group. From the investigation, it was concluded that Nrf2 played a crucial role in bone regeneration. Thus, it was suggested that modulating Nrf2 activity could have a potential therapeutic effect in fracture healing.
Evaluation of the effects of a compound on bone healing during distraction osteogenesis
Researchers studied the effects of a specific compound on bone regeneration during distraction osteogenesis in mice. The mice were evaluated under two different dosing regimens, and the results showed a significant decrease in the mineralized area of the bone gap in mice treated with the compound compared to the control group. Further analysis confirmed a significant decrease in cellular bone formation in the treated mice. The study concluded a short-term negative effect of the compound in the bone repair process during distraction osteogenesis.
Evaluation of the effect of a protein on fracture repair
Researchers evaluated the role of a specific protein in fracture healing using genetically modified mice that lacked that protein. The mice underwent tibial shaft fracture, and analysis was performed to investigate the effect of the deficiency on the healing processes of the fracture. X-ray radiographs and micro-CT analysis showed that the knockout mice showed accelerated formation and remodeling of the fracture callus compared to the control group. Regarding biomechanical properties examined using the three-point bending test at weeks 3 and 4 post-fracture, the knockout mice showed greater stiffness at day 21. However, no significant difference could be observed between the knockout and control groups on day 28. Although an increase in the ultimate force was observed in the knockout mice, work to failure required was comparable between both groups at days 21 and 28 post-fracture induction. The investigation suggested that down-regulation of the protein activity could be a potential therapeutic approach for accelerating fracture healing based on the observation of accelerated fracture callus mineralization and up-regulated expression of osteoclastogenic genes in the knockout mice.
Evaluation of the effect of local vibration and pulsed electromagnetic field on bone fracture
Male rats that were subjected to tibial osteotomy were utilized to investigate the possible therapeutic effect of local low-magnitude, high-frequency vibrations (LMHFV) and pulsed electromagnetic field (PEMF) on the bone healing process. A mechanical stimulator was used to conduct vibrations for 15 min/day using the clamp method in the LMHFV group to overcome the limitations of whole-body vibrations. This method allowed control of vibration magnitude and frequency while exposing the tibia to the vibration in a fixed position. For the second group, PEMF treatment was performed each day. Both treatments were started 5 days postoperatively. Analysis of the radiographs taken 21 days after the end of the healing process showed enhanced callus formation, obliteration of the fracture line, and bridging of the fracture gap in the treatment group as compared to the control group. The stereological analysis showed a significant difference in the summed area of the new bone area between all three groups. Further, LMHFV treatment was observed to have preserved more trabecula as opposed to the control group. Statistically, a significant difference was also observed between the three groups in terms of cartilage summed-area. Based on the observations made during the investigations, it was suggested that osteoblasts are sensitive to low-magnitude, high-frequency vibrations.
Investigation of bone fracture healing in splenectomized rats
Splenectomy is required in fracture patients with blunt abdominal trauma and failure of conservative management. Researchers investigated the effect that splenectomy has on the bone healing process using rats that underwent femoral fracture. The subjects were then divided into two groups. One of the groups followed the fracture with splenectomy (fracture + splenectomy) while the other group only underwent spleen isolation (fracture group). Splenectomy was performed by making a vertical incision under the left costal margin and isolating the spleen using blunt forceps. Splenectomy was followed by ligation of blood vessels and subsequent removal of the spleen. The abdominal wall and skin incision were then sutured. Results from the investigation suggested splenectomy inhibited the recruitment of macrophages and the production of inflammatory cytokines. Further, fracture healing was delayed in the splenectomy group as evident from the histological analysis.
Investigation of conjugated linoleic acid in promoting fracture healing
Researchers aimed to investigate the fracture healing capabilities of conjugated linoleic acid (CLA) in rats. The rats were maintained on either a basal-only diet or CLA with a basal diet. The rats were subjected to a standard tibial fracture procedure. CLA effect was quantified using combined structural evaluation, biomechanical test, and histological examination. Radiological evaluation of the fracture healing process was assessed on weeks 2, 4, and 6, and the degree of healing was evaluated. Micro-CT analysis at week 6 revealed the CLA group to have significantly higher values for bone mineral density, bone strength index, and cross-sectional area of the callus. Load-to-failure values of the CLA group as determined by the three-point bending test were also statistically significant. The investigation showed that CLA improved the quality and mechanical strength of fracture healing in rat callus, thus suggesting potential therapeutic applications of CLA in fracture healing.
Evaluation of whole-body vibrations in improving fracture healing in ovariectomy-induced osteoporosis rats
Osteoporosis leads to an imbalance in the bone tissue absorption and replacement, resulting in weaker bones that are prone to fractures. This condition is often accelerated by age and is commonly seen in post-menopausal women. In their investigation, researchers investigated the effect of whole-body vibrations on fracture healing in rats that underwent ovariectomy. For their experiment, researchers used female rats that were divided into ovariectomy and sham groups. Ovariectomy was performed by bilateral extraction of the ovaries through a dorsolateral approach. Sham models only had their ovaries exposed but otherwise left undisturbed. Both groups underwent a closed fracture procedure at mid-femur three months after ovariectomy or sham surgery. Three days following the fracture procedure, rats were subjected to whole-body vibration therapy. Both the ovariectomy and sham group received whole-body vibration therapy over the course of 14 or 28 days. Data from the investigation revealed that ovariectomized rats had significantly lower bone density and bone content in comparison to the controls. However, it was also observed that whole-body vibration therapy partially protected against bone loss in the ovariectomized rats though not in the controls. Data analysis from the investigation suggested that vibration therapy led to the improvement of the quality of the bone and fractured bone callus in ovariectomized rats.
Advantages And Disadvantages Of Rodent Models
In comparison to large animal models such as dogs and sheep, rodent models offer many advantages. Despite their large size being an advantage, the handling and maintenance of large animals are difficult. Additionally, the cost of husbandry is high in comparison to that of rodents. Large animal models also lack the availability of transgenic animals. Rodents, on the other hand, are economical since they are inexpensive and have shorter breeding cycles. Further, rodents are well-researched animals, and much is already documented with respect to their biological processes and responses to diet modifications and the administration of substances. The availability of transgenic and knock-out rodents also makes them a viable choice for different investigations.
However, the rodent skeletal system does have a significant distinction from the human skeleton. Unlike the human skeleton, the rodent skeleton continues to grow and reshape throughout its life cycle. Growth plates in rodents remain open well into their adulthood. With the advancement in age, rodents show loss of cancellous bone, thinning of cortical bone, and increased cortical porosity as seen in humans. Their reduced lifespan makes them ideal for studies investigating the effects of aging on bone metabolism and regeneration processes. Rodents so require working within their biological constraints and their small size may also not be suitable for modeling certain orthopedic investigations. Their use in chondral defect repair investigations is limited due to the thinness of their cartilage layer. Rodents also vary significantly from humans in their gait pattern and biomechanical loading environment.
Summary
Orthopedic research involves the improvement of treatments of musculoskeletal system conditions. Rodent models are preferred over large animal models due to their low maintenance and cost, shorter breeding cycles, and faster regeneration. The availability of transgenic and knock-out rodents makes them ideal for various research requirements. The reduced lifespan of rodents allows age-dependent investigation. Rodents show loss of cancellous bone, thinning of cortical bone, and increased cortical porosity with age as seen in humans. Rodent strain, age, and weight among other factors influence orthopedic investigations. Anesthesia induction can be done using inhalants or injectable agents. The depth of anesthesia should be verified before beginning surgical procedures. During surgical procedures, care must be taken not to damage surrounding tissues or bones. A recovery area should be set up, and fluids should be replaced by subcutaneous or intraperitoneal injection of warm sterile saline. Infections may influence the results of the investigation; hence, euthanizing the subject is recommended should it occur. Appropriate pain management techniques should be followed.
References
- Bilgin HM, Çelik F, Gem M, Akpolat V, Yıldız İ, Ekinci A, Özerdem MS, Tunik S (2017). Effects of local vibration and pulsed electromagnetic field on bone fracture: A comparative study. Bioelectromagnetics. 38(5):339-348. doi: 10.1002/bem.22043.
- Bonnarens F, Einhorn TA (1984). Production of a standard closed fracture in laboratory animal bone. J Orthop Res. 1984;2(1):97-101.
- Bove SE, Laemont KD, Brooker RM, Osborn MN, Sanchez BM, Guzman RE, Hook KE, Juneau PL, Connor JR, Kilgore KS (2006). Surgically induced osteoarthritis in the rat results in the development of both osteoarthritis-like joint pain and secondary hyperalgesia. Osteoarthritis Cartilage. 14(10):1041-8.
- Butezloff MM, Zamarioli A, Leoni GB, Sousa-Neto MD, Volpon JB (2015). Whole-body vibration improves fracture healing and bone quality in rats with ovariectomy-induced osteoporosis. Acta Cir Bras. 2015 Nov;30(11):727-35. doi: 10.1590/S0102-865020150110000002.
- Gomes PS, Fernandes MH (2011). Rodent models in bone-related research: the relevance of calvarial defects in the assessment of bone regeneration strategies. Lab Anim. 45(1):14-24. doi: 10.1258/la.2010.010085.
- Haffner-Luntzer M., Kovtun A., Rapp A.E, Ignatius A. (2016). Mouse Models in Bone Fracture Healing Research. Curr Mol Bio Rep. 2: 101. https://doi.org/10.1007/s40610-016-0037-3
- Jung YJ, Kim R, Ham HJ, Park SI, Lee MY, Kim J, Hwang J, Park MS, Yoo SS, Maeng LS, Chang W, Chung YA (2015). Focused low-intensity pulsed ultrasound enhances bone regeneration in rat calvarial bone defect through enhancement of cell proliferation. Ultrasound Med Biol. 41(4):999-1007. doi: 10.1016/j.ultrasmedbio.2014.11.008.
- Kogan NM, Melamed E, Wasserman E, Raphael B, Breuer A, Stok KS, Sondergaard R, Escudero AV et al., (2015) Cannabidiol, a Major Non-Psychotropic Cannabis Constituent Enhances Fracture Healing and Stimulates Lysyl Hydroxylase Activity in Osteoblasts. J Bone Miner Res. 30(10):1905-13. doi: 10.1002/jbmr.2513.
- Lippross S, Beckmann R, Streubesand N, Ayub F, Tohidnezhad M, Campbell G, Kan YW, Horst F, Sönmez TT, Varoga D, Lichte P, Jahr H, Pufe T, Wruck CJ (2014). Nrf2 deficiency impairs fracture healing in mice. Calcif Tissue Int. 95(4):349-61. doi: 10.1007/s00223-014-9900-5.
- Lybrand K, Bragdon B, Gerstenfeld L (2015). Mouse models of bone healing: fracture, marrow ablation, and distraction osteogenesis. Curr Protoc Mouse Biol. 5(1):35-49. doi: 10.1002/9780470942390.mo140161.
- Moran CJ, Ramesh A, Brama PA, O’Byrne JM, O’Brien FJ, Levingstone TJ (2016). The benefits and limitations of animal models for translational research in cartilage repair. J Exp Orthop. 3(1):1. doi: 10.1186/s40634-015-0037-x.
- Powers DL, Claassen B, Black J (1995). The rat as an animal model for total hip replacement arthroplasty. J Invest Surg. 8(5):349-62.
- Shan Z, Luo ZP, Shen X, Chen L (2017). Promotion of fracture healing by conjugated linoleic acid in rats. J Orthop Surg (Hong Kong). 25(2):2309499017718910. doi: 10.1177/2309499017718910.
- Spicer PP, Kretlow JD, Young S, Jansen JA, Kasper FK, Mikos AG (2012). Evaluation of bone regeneration using the rat critical size calvarial defect. Nat Protoc. 7(10):1918-29. doi: 10.1038/nprot.2012.113.
- Stine KC, Wahl EC, Liu L, Skinner RA, Vanderschilden J, Bunn RC, Montgomery CO, Suva LJ, Aronson J, Becton DL, Nicholas RW, Swearingen CJ, Lumpkin CK Jr (2014). Cisplatin inhibits bone healing during distraction osteogenesis. J Orthop Res. 2014 Mar;32(3):464-70. doi: 10.1002/jor.22527
- Wang D, Gilbert JR, Cray JJ Jr, Kubala AA, Shaw MA, Billiar TR, Cooper GM (2012). Accelerated calvarial healing in mice lacking Toll-like receptor 4. PLoS One. 7(10):e46945. doi: 10.1371/journal.pone.0046945.
- Xiao W, Hu Z, Li T, Li J (2017). Bone fracture healing is delayed in splenectomic rats. Life Sci. 173:55-61. doi: 10.1016/j.lfs.2016.12.005.
- Xie Y, Luo F, Xu W, Wang Z, Sun X, Xu M, Huang J, Zhang D, Tan Q, Chen B, Jiang W, Du X, Chen L (2017). FGFR3 deficient mice have accelerated fracture repair. Int J Biol Sci. 2017 Jul 18;13(8):1029-1037. doi: 10.7150/ijbs.19309.
- Xiong, C., Zhang, Z., Baht, G. S., Terrando, N (2018). A Mouse Model of Orthopedic Surgery to Study Postoperative Cognitive Dysfunction and Tissue Regeneration. J. Vis. Exp. (132), e56701, doi:10.3791/56701.



































































Reviews
There are no reviews yet.