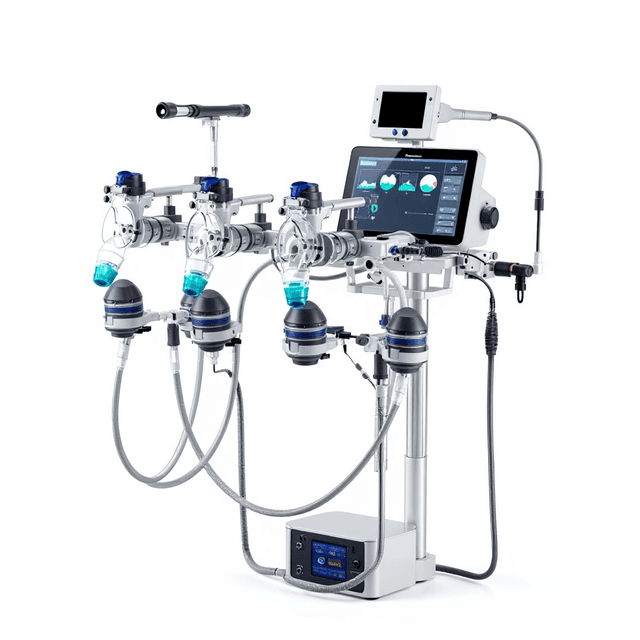
Intelligent Anesthesia Ventilator
Precision mechanical ventilator for laboratory animals up to 100kg, featuring programmable tidal volume (20-1500ml), respiration rate control, and dual bellows system with touchscreen interface.

Louise Corscadden, PhD
Director of Science · ConductScience
Ask Louise about Intelligent Anesthesia Ventilator fit, setup, configuration, or quote prep.
Already working with us? Sign in to connect this with My Scientist.
Key Specifications
Full details →- Model fit
- up to 100 kg
- SKU family
- CS-958448
- Sizing
- 52.0 x 36.0 x 37.0 cm
- Ordering
- Online checkout and quote request available
- Category
- Anesthesia & Ventilation
- Build notes
- Confirm accessories, station layout, and support needs before purchase
R419/R420 intelligent ventilator callouts
- Modes: VCV, PIPCV, and APNEA with built-in dog/cat presets so entering weight auto-calculates RR, VT, and PIP.
- Delivery range: 20-1,500 mL tidal volumes, 2-60 BPM, and 5-35 cmH2O peak inspiratory pressure with trigger sensitivity down to -9 cmH2O.
- Hardware: 5" 800x480 touch display, 20-300 mL and 300-1,500 mL bellows, internal battery (~4 h), and 3.22 kg footprint (253 x 224 x 112 mm).
The list price is now $4,280 to stay aligned with direct RWD partner quotes while still covering bench QA and inbound freight.
Datasheet: RWD intelligent ventilator page
The Intelligent Anesthesia Ventilator is a precision mechanical ventilation system designed for laboratory animals and research applications requiring controlled respiratory support. This compact ventilator delivers intermittent positive pressure ventilation (IPPV) with programmable respiratory parameters including tidal volume (20-1500ml), respiration rate (2-60 bpm), and inspiratory/expiratory ratios (1:1.1 to 1:4.0). The system features dual bellows capacity ranges (0-300ml and 300-1500ml) to accommodate subjects from small laboratory animals to large research models up to 100kg body weight.
The ventilator incorporates a 5-inch color touchscreen interface (800×480 resolution) for parameter programming and real-time monitoring of proximal airway pressure. The system includes dual LED and sound alarm capabilities for safety monitoring during procedures. Compatible with standard laboratory gas supplies (O2, nitrogen, and clean dry air) at operating pressures of 41-87 PSI, this ventilator supports both anesthesia protocols requiring respiratory depression management and surgical procedures utilizing neuromuscular blocking agents.
How It Works
The Intelligent Anesthesia Ventilator operates on the principle of intermittent positive pressure ventilation (IPPV), delivering predetermined volumes of gas mixture directly to the subject's airways at controlled pressures and timing intervals. The system utilizes two interchangeable bellows chambers - a small capacity bellows (0-300ml) for smaller subjects and a large capacity bellows (300-1500ml) for larger animals - to generate precise tidal volumes calculated at approximately 7-10ml per kilogram of body weight.
Gas delivery is controlled through programmable inspiratory and expiratory phases, with adjustable I:E ratios from 1:1.1 to 1:4.0 to accommodate different physiological requirements. The system monitors real-time proximal airway pressure to ensure safe delivery pressures between 5-35 cmH2O peak inspiratory pressure, while trigger pressure sensitivity (-9.0 to -1.0 cmH2O) allows for assisted ventilation modes when subjects retain some spontaneous respiratory effort.
The ventilator accepts standard laboratory gas supplies (oxygen, nitrogen, or clean dry air) at supply pressures of 41-87 PSI, with internal pressure regulation ensuring consistent delivery parameters regardless of source pressure variations. The integrated monitoring system provides continuous feedback on respiratory parameters through the touchscreen interface while dual alarm systems (LED and audible) alert operators to pressure deviations or system malfunctions.
Features & Benefits
animal_weight_capacity
- up to 100 kg
bellows_capacity_small
- 0 to 300 ml
bellows_capacity_large
- 300 to 1500 ml
tidal_volume_calculation
- approximately 7 to 10 ml/kg body weight
alarm_system
- dual LED and sound alarm
pressure_monitoring
- real-time proximal airway pressure
gas_supply_compatibility
- O2, nitrogen, and clean, dry air
ventilation_type
- intermittent positive pressure ventilation (IPPV)
included_bellows
- two interchangeable bellows
Power Supply
- 100-220V
- 100-240V
Automation Level
- semi-automated
Power/Voltage
- 100-220V
- 100-240V
Species
- Dog
- Non-human Primate
- Pig
- Rabbit
Display Type
- LED
Weight
- 5.8 kg
Dimensions
- 22.5 cm x 2.8 cm x 3.2 cm
Research Domain
- Cancer Research
- Cardiovascular
- Developmental Biology
- Neuroscience
- Pain Research
- Toxicology
Weight
- 18.96 kg
Dimensions
- L: 52.0 mm
- W: 36.0 mm
- H: 37.0 mm
| Feature | This Product | Typical Alternative | Advantage |
|---|---|---|---|
| Tidal Volume Range | 20-1500ml with dual bellows system | Fixed bellows models often limited to single capacity range | Single ventilator accommodates complete range of laboratory animal sizes without equipment changes. |
| Display Interface | 5-inch color touchscreen (800×480 resolution) | Basic models use LED readouts or analog gauges | Intuitive programming interface reduces setup time and parameter adjustment errors. |
| I:E Ratio Adjustment | Continuously adjustable from 1:1.1 to 1:4.0 | Entry-level units offer fixed or limited ratio options | Precise control over respiratory timing enables optimization for specific experimental protocols. |
| Pressure Monitoring | Real-time proximal airway pressure with dual alarms | Basic models may lack continuous monitoring capabilities | Continuous pressure feedback ensures subject safety and enables immediate response to airway changes. |
| Weight and Portability | 3.22kg in compact 253×224×112mm housing | Larger bench-top models often exceed 10kg | Enhanced portability allows ventilator relocation between surgical suites without equipment carts. |
This ventilator combines dual bellows flexibility with touchscreen control and comprehensive pressure monitoring in a compact, portable design. The system provides research-grade ventilation capabilities while maintaining the mobility and ease of use required for diverse laboratory environments.
| Model | SKU | Listed price | Status | Dimensions |
|---|---|---|---|---|
| 100-240V | RWD-VPR419 | $4,600.00 | Available | 52.0 x 36.0 x 37.0 cm |
| 100-220V | RWD-VLR419 | $4,600.00 | Available | 52.0 x 36.0 x 37.0 cm |
Practical Tips
Verify tidal volume accuracy using a calibrated spirometer before each experimental series, especially when switching between bellows assemblies.
Why: Ensures precise volume delivery critical for consistent experimental conditions and subject safety.
Clean and inspect bellows assemblies for wear or damage after each use, replacing seals if compression efficiency decreases.
Why: Maintains volume accuracy and prevents pressure leaks that could compromise ventilation effectiveness.
Calculate and program tidal volume at 7-10ml/kg body weight, then fine-tune based on blood gas analysis results during longer procedures.
Why: Optimizes gas exchange while preventing over-ventilation that could affect experimental parameters.
If pressure alarms activate frequently, check breathing circuit connections and endotracheal tube patency before adjusting pressure limits.
Why: Identifies mechanical issues that could compromise ventilation rather than masking problems with parameter changes.
Record baseline pressure readings and ventilation parameters at procedure start for comparison during post-procedure analysis.
Why: Provides reference data for assessing respiratory changes and validating experimental conditions.
Set peak inspiratory pressure limits 5-10 cmH2O below maximum to allow safety margin for pressure spikes during subject movement.
Why: Prevents barotrauma while maintaining adequate ventilation during periods of increased airway resistance.
Allow 2-3 minutes stabilization time after parameter changes before beginning experimental measurements.
Why: Ensures new ventilation settings have reached steady-state conditions for consistent data collection.
Setup Guide
What’s in the Box
- Intelligent Anesthesia Ventilator main unit
- Small capacity bellows (0-300ml)
- Large capacity bellows (300-1500ml)
- Power cord (100-220V)
- Gas supply connection tubing (typical)
- User manual and quick reference guide (typical)
- Calibration certificate (typical)
Warranty
ConductScience provides a standard one-year manufacturer warranty covering defects in materials and workmanship, with comprehensive technical support for installation, calibration, and operational guidance.
Compliance
How do I determine the appropriate tidal volume for different animal weights?
Calculate tidal volume at approximately 7-10ml per kilogram of body weight. The system's dual bellows design (0-300ml for smaller animals, 300-1500ml for larger subjects) accommodates this range while maintaining precise volume delivery.
What gas supply pressures and types are compatible with this ventilator?
The system accepts oxygen, nitrogen, or clean dry air at supply pressures between 41-87 PSI. Internal pressure regulation ensures consistent delivery regardless of source pressure variations within this range.
How does the trigger pressure function work for assisted ventilation?
Trigger pressure sensitivity ranges from -9.0 to -1.0 cmH2O, allowing the ventilator to detect spontaneous respiratory efforts and provide assisted breaths when subjects retain some natural breathing capacity.
What safety monitoring features are included during operation?
The system provides real-time proximal airway pressure monitoring with dual LED and sound alarms that activate when pressure parameters exceed safe limits or system malfunctions occur.
Can the I:E ratio be adjusted for different experimental protocols?
Yes, inspiratory to expiratory ratios are adjustable from 1:1.1 to 1:4.0 to accommodate various physiological requirements and experimental designs requiring specific breathing patterns.
What is the maximum subject weight this ventilator can support?
The system is designed for subjects weighing up to 100kg, with the large capacity bellows (300-1500ml) providing adequate tidal volumes for larger research animals.
How portable is this ventilator for multi-location use?
With dimensions of 253×224×112mm and weight of 3.22kg, the unit is highly portable for transport between surgical suites or experimental locations within a facility.
Have a question about this product?
Have a question? Just ask.
Send it over and we'll email you a personalized answer — no call, no scheduling.
Prefer to talk it through?
Accessories
Enhance your setup with compatible accessories